Craniosyntosis
An infant’s skull is made up of lots of interlocking bones that will join later, allowing for brain growth. Craniosynostosis (CS) is a premature fusion of one or more of these joining points, called cranial sutures. It causes a deformation of the skull. The incidence of CS is difficult to quantify since some milder forms are not reported, but our best estimates are roughly one baby in 2,100 is born with it. With CS, the head and brain growth can be restricted depending on the number and location of the suture fusion. CS requires surgery to be corrected and often a remolding helmet is added depending on the age of the child. Premature fusion of one or more of these sutures causes abnormal growth patterns perpendicular to the suture, resulting in changes to the infant head shape and at times the face of the infant.
Plain x-rays are generally not helpful in the diagnosis of craniosynostosis. If the health care professional is unsure of the diagnosis, a 3-D CT scan of the skull may help. A 3-D CT is done in a regular CT scanner but takes many more pictures of the skull. The baby or child is required to lay still, so depending on the age of the child, sedation may or may not be necessary. Computer software is then used to create a 3-D model of the skull, which is useful for both diagnosis and surgical planning. In some cases, mostly with multiple suture synostosis, the neurosurgeon may order an MRI of the brain to check the overall health of the brain and to make sure there is not underlying hydrocephalus before any operations are performed.
What causes craniosynostosis?
Craniosynostosis may be caused by genetic factors. Most cases of craniosynostosis are not related to a genetic abnormality. Certain suture fusions are more likely to have a genetic cause than others and thought to have a genetic link as they tend to be found in more than one family member. For some instances of craniosynostosis a single-gene mutation is likely to be the cause. These gene mutations cause early fusing of the normal sutures of the skull.
Syndromic or multiple suture synostosis is often caused by multiple gene mutations which may include FGFR 1, FGFR 2, FGFR 3 and the TWIST genes. Mutation of these genes can lead to the more severe forms of craniosynostosis such as Crouzons, Apert and Peiffer syndromes.
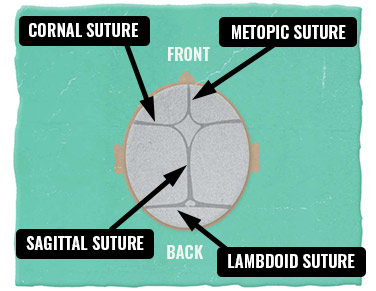
Normal Sutures
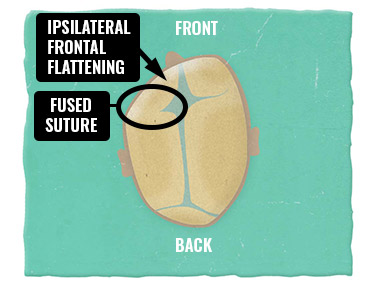
Unilateral coronal syntosis
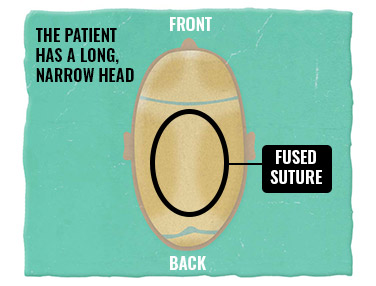
Saggital syntosis
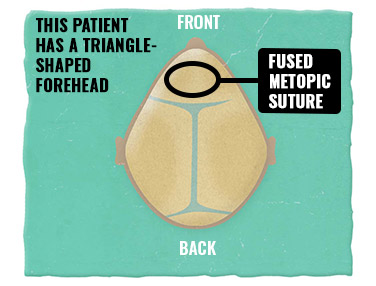
Metopic syntosis
How is craniosynotosis diagnosed?
Most often, craniosynostosis is diagnosed by a thorough physical exam. This helps to distinguish a craniosynostosis from a positional head shape abnormality such as positional plagiocephaly or brachycephaly. There are tell-tale signs that help clinicians determine the type of craniosynostosis:
Sagittal synostosis:
This is a premature fusion of the sagittal suture. Fusion of this suture does not allow for the expansion of the skull width-wise and so the babies develop long narrow heads. Sometimes the infants will develop what is known as “frontal bossing” or a forehead that seems to stick out more than that of the average baby. In these babies the back part of the head will tend to be narrower than the forehead, which is not the case in a normal infant skull where the back part of the head is the widest part of the skull.
Coronal synostosis (unilateral or bilateral):
Coronal synostosis can be the fusion of one of the coronal sutures (unilateral) or fusion of both sutures (bilateral). Unilateral coronal synostosis will cause one eye to look significantly wider than the other and will cause the nose to tip to one side. Bilateral coronal synostosis (both sides) will give the appearance of a very tall forehead and two wide eyes and is more likely to be associated with an underlying genetic abnormality.
Metopic synostosis:
Metopic synostosis is a premature fusion of the suture line that runs down the middle of the forehead. It gives the appearance of a triangular forehead and the eyes are close together. Because the metopic suture normally fuses at a young age, this type of synostosis is generally not progressive and the look of the forehead and face will usually not get worse over time.
Lambdoid synostosis:
Lambdoid synostosis is very rare and is often confused with a positional plagiocephaly. Lambdoid synostosis causes a flat back of the head on the same side as the fused suture. The ear on the fused side tends to be located more downwards and backwards than the other ear.
Plain x-rays are generally not helpful in the diagnosis of craniosynostosis. If the health care professional is unsure of the diagnosis, a 3-D CT scan of the skull may help. A 3-D CT is done in a regular CT scanner but takes many more pictures of the skull. The baby or child is required to lay still, so depending on the age of the child, sedation may or may not be necessary. Computer software is then used to create a 3-D model of the skull, which is useful for both diagnosis and surgical planning. In some cases, mostly with multiple suture synostosis, the neurosurgeon may order an MRI of the brain to check the overall health of the brain and to make sure there is not underlying hydrocephalus before any operations are performed.
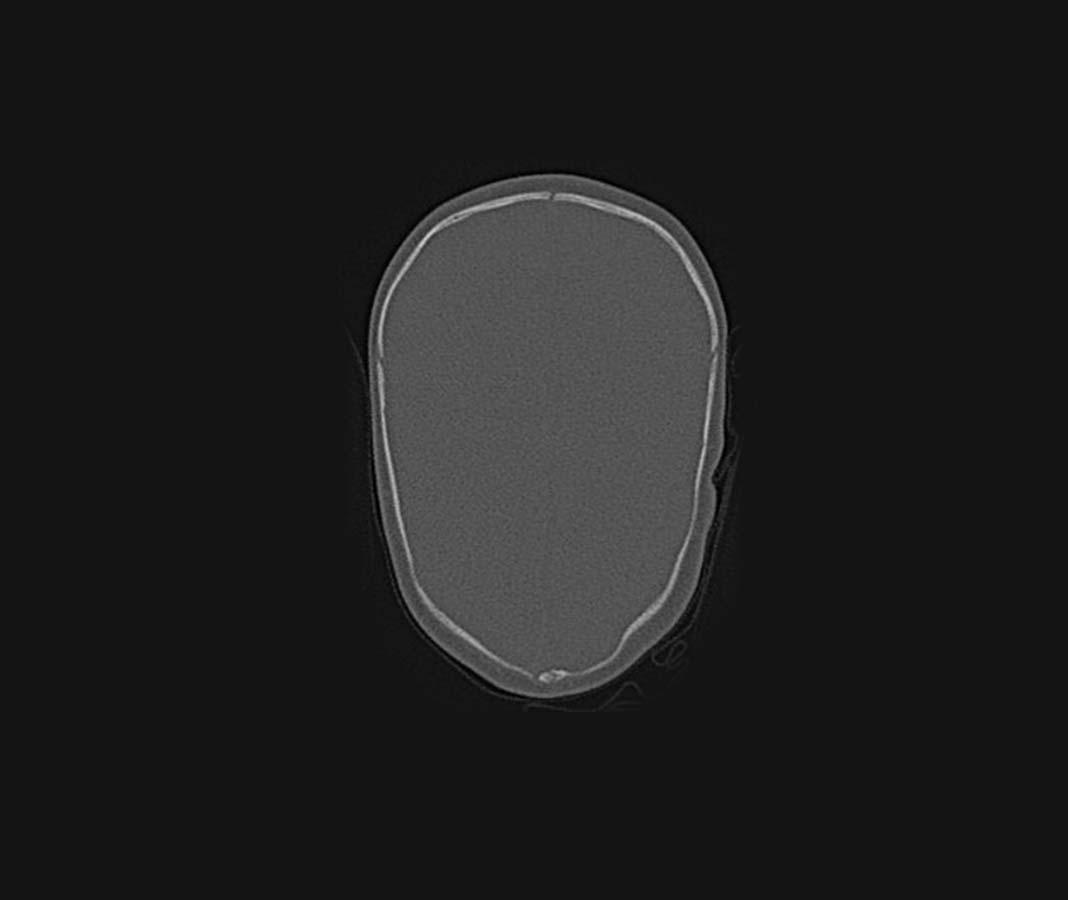
Regular CT showing bone
How is craniosynostosis treated?
There are several ways to approach the correction of craniosynostosis. Options for surgery depend on the age and diagnosis of your child. Different centres may offer different treatment options. At the Stollery Children’s Hospital we generally have three different types of surgical repairs:
Endoscopic surgical repair:
This surgery is most commonly available to babies under three to four months of age that have a sagittal synostosis. While there may be options to perform endoscopic surgery on a different fused suture, such as a lambdoid or a unilateral coronal, the infant age is not optional. In order to be able to perform this surgery endoscopically the bone of the infant’s skull must be thin enough to use scissors to cut it. After four months of age the child’s skull changes, making the technique less effective. If your baby is a candidate for an endoscopic repair, they will have two three-centimetre incisions on the scalp, one just behind the soft spot or fontanel and a second incision near the back of their skull.
Using an endoscope, the scalp is carefully lifted off the skull so as to not tear any major veins. Surgical scissors are then used to cut out at the fused suture, which is approximately the width of your thumb and about eight to 10 centimetres long. Cuts may also be made under the skin down the sides of the skull to allow for more rapid growth width wise. The surgery takes about two to three hours to complete. Babies often spend their first night after the operation in the ICE room (intermediate care environment) or step-down PICU (pediatric intrusive care unit) and are in hospital for two days. At this age the bone that is removed will grow back in, much like the soft spot of a baby closes as the baby gets older.
Once the skin incisions have healed, approximately two weeks after the surgery, the baby will be fitted for a remolding helmet. This helmet will continue to round out the skull, and works by gradual pressure, much like a retainer does on a child’s mouth. The helmet is worn 23 hours a day, seven days a week, for four to six months. The helmet must be modified here at the Stollery Children’s Hospital every week for the first months, and then approximately every two weeks after that. Occasionally a second helmet may need to be made if the head growth or skull shape change is rapid and the baby outgrows the current helmet. There are no out-of-pocket costs associated with the surgery or helmets for babies who have craniosynostosis.
Minimal open surgical repair:
This surgery is similar to the endoscopic surgical repair, but will often have wider incisions as either the forehead, the back of the head or both are more severe and require more surgical repair. This still requires the infant to be under about eight months of age and to have only one fused suture. The surgery takes about two to three hours to complete, babies often spend their first night after the operation in the ICE room or step-down PICU and are in hospital for two to four days. Most babies will require a remolding helmet after the surgery.
Total cranial vault repair:
This surgery is often performed on infants who are diagnosed older or have multiple suture fusions. A total cranial vault involves an ear-to-ear incision and will most likely require some dissolvable plates and screws to be used to secure the bone cuts in place. The surgery varies from case to case. Occasionally the neurosurgeons will ask a pediatric plastic surgeon to help with shaping the skull. This surgery takes six to eight hours, and infants may spend a night in the Pediatric Intensive Care before being transferred to the ICE room or step-down PICU. Generally, babies are in hospital for about a week and usually they do not require a remolding helmet.
Reference:
Hummel, P., & Fortado, D. (2005a). “Impacting Infant Head Shapes. Advances in Neonatal Care,” 5(6), 329-340.
Lajeunie, E., Le Merrer, M., Bonaiti-Pellie, C., Marchac, D., & Renier, D. (1995). Genetic study of nonsyndromic coronal craniosynostosis. American Journal of Medical Genetics, 55(4), 500-504.
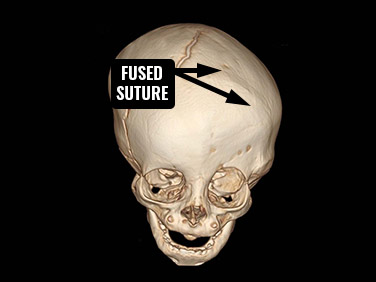
3D CT scan showing fused LT coronal suture
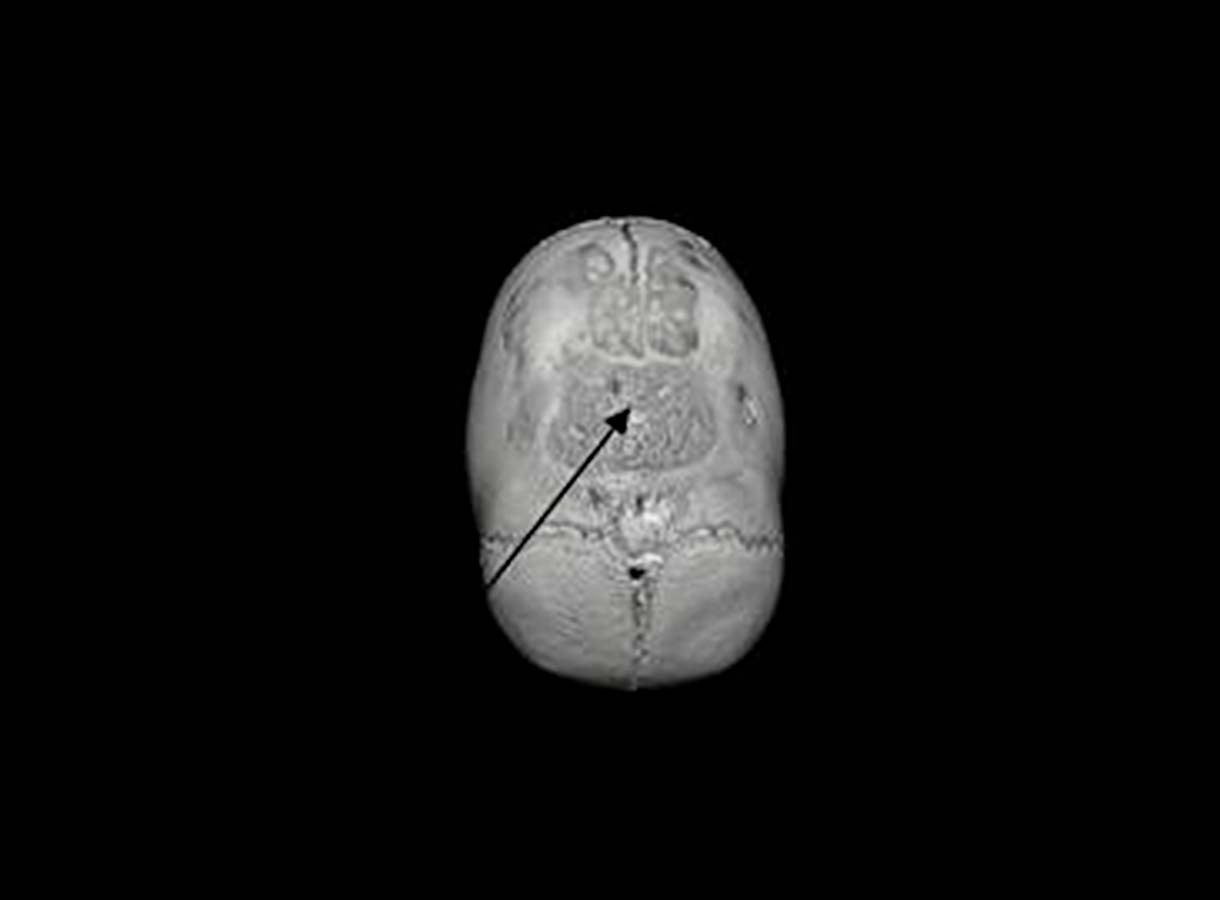
3D CT scan showing a fused sagittal suture
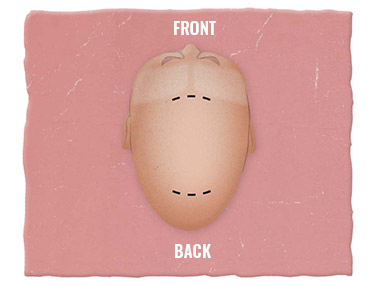
Endoscopic sagittal syntosis repair-incisions
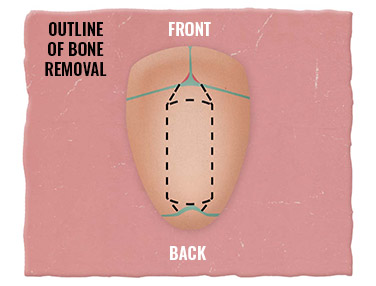
Endoscopic sagittal syntosis repair-removal